Skyrizi Enrollment Form Printable
Skyrizi Enrollment Form Printable - The hcp and the patient or legally authorized person should fill out this form completely before leaving. Go to myaccredopatients.com to log in or get started. Tell your healthcare provider about all the medicines you take, including prescription and o. Through this form, patients can apply for. Skyrizi complete is a program that offers support, savings, and guidance for patients taking skyrizi, a prescription medicine for psoriasis, psoriatic arthritis, and crohn's disease. Four simple steps to submit your referral. The categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information. This file contains the enrollment and prescription form for the skyrizi treatment program. The information you provide will be used by a pharmacy affiliated with janssen biotech, inc., and. Please provide copies of front and back of all medical and prescription insurance cards. Edit your skyrizi enrollment form online. Tell your healthcare provider about all the medicines you take, including prescription and o. When faxing this form, please include the patient demographic sheet, ensuring the. O ulcerative colitis maintenance phase, administer skyrizi: — to be faxed by infusion provider with the enrollment form. Four simple steps to submit your referral. Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the prescription process for your patients. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Through this form, patients can apply for. It includes information on enrollment, important safety. O 180mg sq at week 12 and every 8 weeks therafter. Edit your skyrizi enrollment form online. Up to 40% cash back send skyrizi enrollment form 2024 via email, link, or fax. When faxing this form, please include the patient demographic sheet, ensuring the. Four simple steps to submit your referral. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Please provide copies of front and back of all medical and prescription insurance cards. Through this form, patients can apply for. This file contains the enrollment and prescription form for the skyrizi treatment program. This file provides essential resources and guidance for skyrizi users. O ulcerative colitis maintenance phase, administer skyrizi: Submit this enrollment form to the dispensing pharmacy as my signature. It provides important information on how to fill out the form and key processes involved in. Please note that the only secure way to transfer this. Please submit the patient authorization form with this completed patient enrollment form. This file provides essential resources and guidance for skyrizi users. Four simple steps to submit your referral. When faxing this form, please include the patient demographic sheet, ensuring the. It provides important information on how to fill out the form and key processes involved in. O 180mg sq at week 12 and every 8 weeks therafter. Go to myaccredopatients.com to log in or get started. O 180mg sq at week 12 and every 8 weeks therafter. Sections in blue (1, 2, 3, 4) denote fields required for enrollment in skyrizi complete. Submit this enrollment form to the dispensing pharmacy as my signature. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. When faxing this form, please include the patient demographic sheet, ensuring the following patient information is included: Edit your skyrizi enrollment form online. Skyrizi complete is a program that offers support, savings, and guidance for patients taking skyrizi, a prescription medicine for psoriasis, psoriatic arthritis, and crohn's disease. Submit this enrollment form to the dispensing pharmacy as my signature. Through. The hcp and the patient or legally authorized person should fill out this form completely before leaving. The categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information. By signing this form, i am authorizing twelvestone health partners and afiliates to serve as my designated agent in submitting prior authorizations and. Four simple steps to submit your referral. Please note that the only secure way to transfer this. Available to patients with commercial. By signing this form, i am authorizing twelvestone health partners and afiliates to serve as my designated agent in submitting prior authorizations and other clinically required. The information you provide will be used by a pharmacy affiliated with. The categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information. Please note that the only secure way to transfer this. This file contains the enrollment and prescription form for the skyrizi treatment program. — to be faxed by infusion provider with the enrollment form. Sections in blue (1, 2, 3,. Up to 40% cash back send skyrizi enrollment form 2024 via email, link, or fax. This file contains the enrollment and prescription form for the skyrizi treatment program. O 180mg sq at week 12 and every 8 weeks therafter. Go to myaccredopatients.com to log in or get started. Completepro.com enables seamless enrollment in skyrizi complete and helps streamline the prescription. Please submit the patient authorization form with this completed patient enrollment form. Up to 40% cash back send skyrizi enrollment form 2024 via email, link, or fax. Four simple steps to submit your referral. O 360mg sq at week 12 and every 8 weeks therafter. O 180mg sq at week 12 and every 8 weeks therafter. Edit your skyrizi enrollment form online. Available to patients with commercial. When faxing this form, please include the patient demographic sheet, ensuring the. The hcp and the patient or legally authorized person should fill out this form completely before leaving. The categories of personal information collected in this enrollment and prescription form include contact, insurance, prescription, and medical history information. Skyrizi complete is a program that offers support, savings, and guidance for patients taking skyrizi, a prescription medicine for psoriasis, psoriatic arthritis, and crohn's disease. 1 patient demographic sheet*—to be faxed by hcp with the enrollment and prescription form. Go to myaccredopatients.com to log in or get started. Please note that the only secure way to transfer this. You can also download it, export it or print it out. It provides important information on how to fill out the form and key processes involved in.
Skyrizi (risankizumab) PSP Formulaire d’inscription AbbVie Care 2022

Skyrizi Enrollment Form Printable
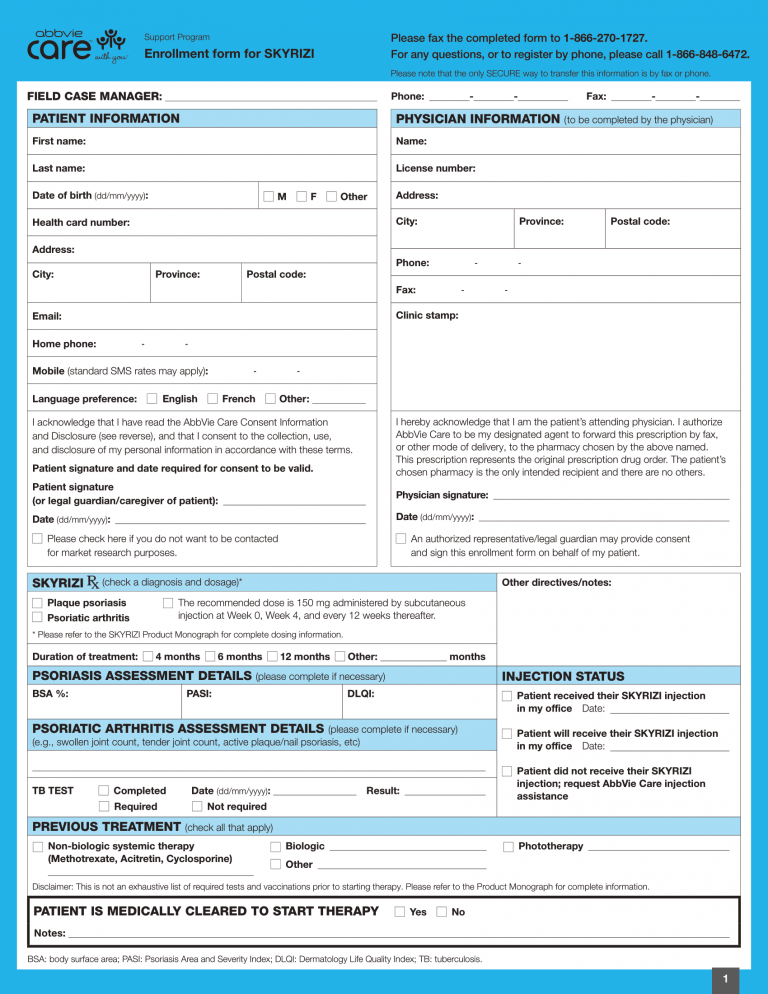
Skyrizi (risankizumab) PSP Form AbbVie Care 2022 EN World OSCAR

Fillable Online Skyrizi (risankizumabrzaa) request form Fax Email

Fillable Online Skyrizi IV CCRD Prior Authorization Form. Prior

Skyrizi Enrollment Form Printable
SKYRIZI® (risankizumabrzaa) for Psoriatic Arthritis

Fillable Online Prescription & Enrollment Form Skyrizi (risankizumab
Skyrizi Enrollment Form Printable, Please complete and fax this form
Skyrizi Enrollment Form Printable
It Includes Information On Enrollment, Important Safety.
Through This Form, Patients Can Apply For.
O Ulcerative Colitis Maintenance Phase, Administer Skyrizi:
— To Be Faxed By Infusion Provider With The Enrollment Form.
Related Post: