Printable Aflac Claim Forms
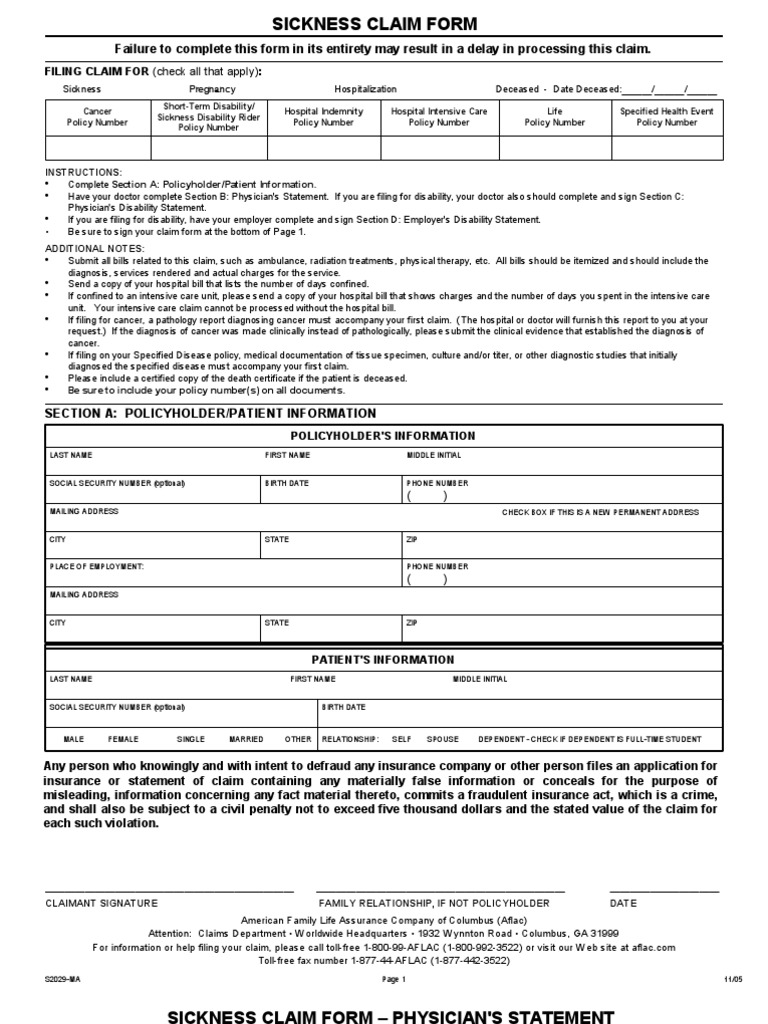
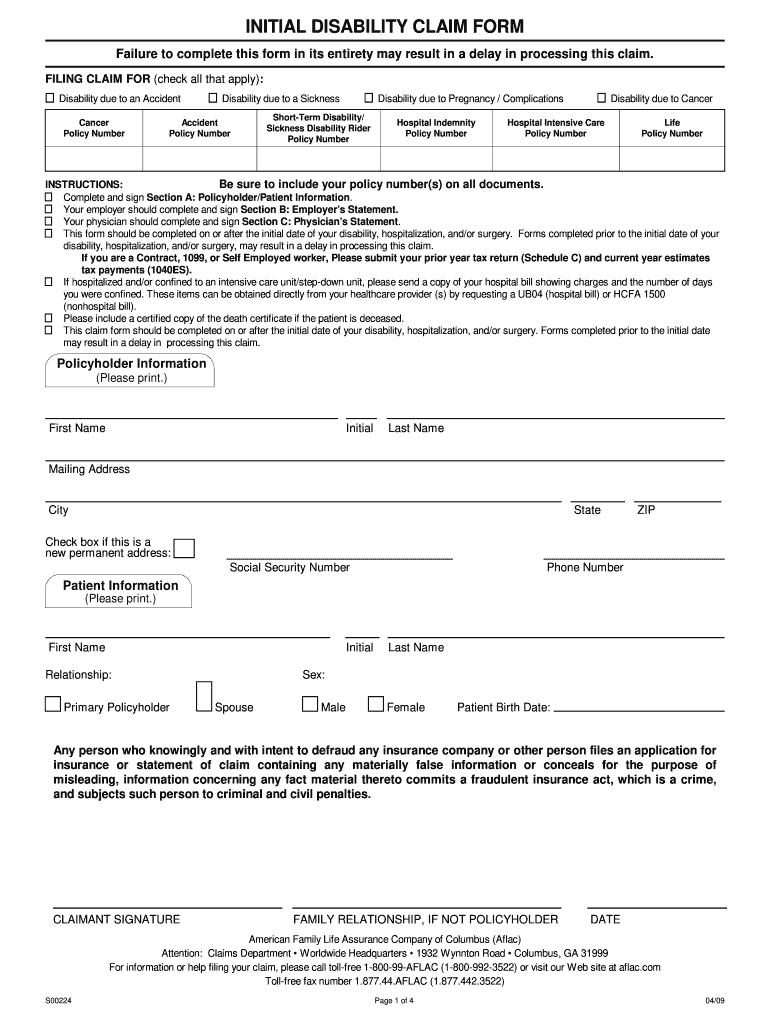
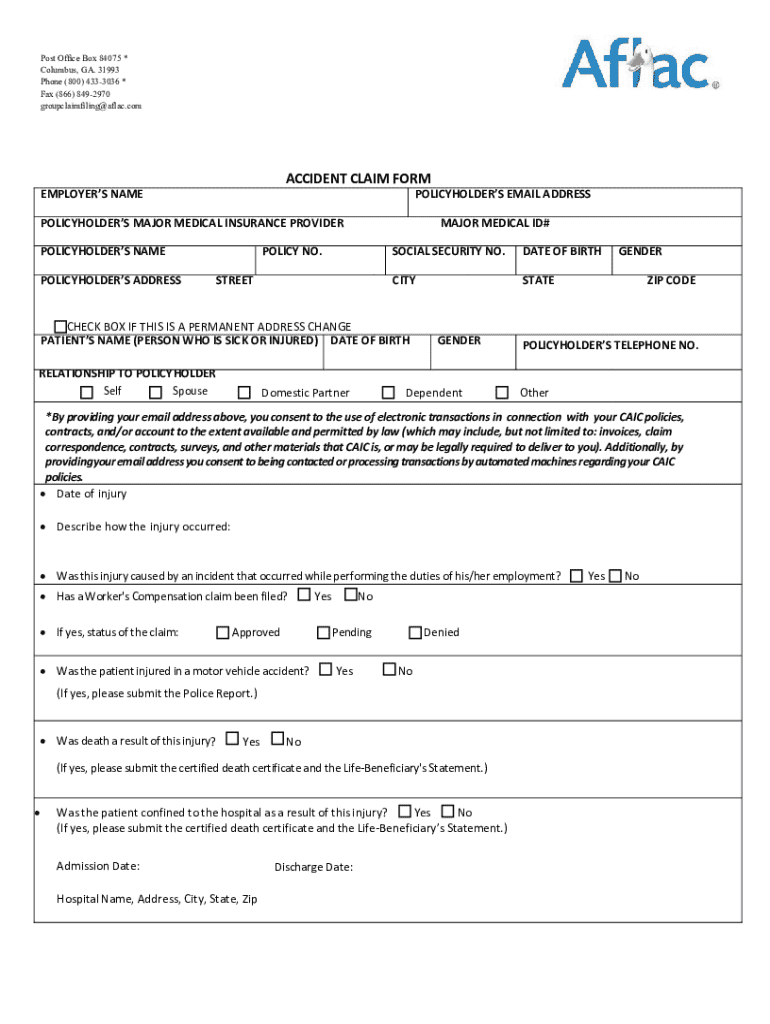
Printable Aflac Claim Forms - Any person who knowingly and with intent to defraud any insurance company, files a statement of claim containing any materially false, incomplete or misleading information, is guilty of a crime. Fill in the policy number, policyholder information, patient information, treatment and physician. Submit only one treatment date per claim form. Please review your policy for specific benefits covered under. Follow these five easy steps to file a claim and get paid fast: To prevent processing delays, please have claim form completed in full and return the signed Download and complete this form to file a claim for hospitalization or surgery. Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. We're here to help you. Accident wellness benefit claim form. Download and print this form to file a claim for wellness benefits under your aflac policy. American family life assurance company of columbus (aflac) attention: Schedule and complete your checkup or screening with your doctor. To prevent processing delays, please have claim form completed in full and return the signed Fill out the required information and submit the form with supporting documentation to aflac for. Failure to complete all sections may result in a delay in processing this claim. Accident wellness benefit claim form. Please review your policy for specific benefits covered under. Fill in the policy number, policyholder information, patient information, treatment and physician. Attach supporting documentation, such as bills, reports, and authorization forms, and email or fax it to aflac. Claims for all other benefits covered under your. Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. Download and print this form to file a claim for wellness benefits under your aflac policy. What type of coverage are you filing a claim? Aflac group makes it easy to file a claim. Follow these five easy steps to file a claim and get paid fast: Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. Download and print this form to file a claim for wellness benefits under your aflac policy. Any person who knowingly and with intent to defraud any insurance company, files a. Any person who knowingly and with intent to defraud any insurance company, files a statement of claim containing any materially false, incomplete or misleading information, is guilty of a crime. Each of our representatives is. Schedule and complete your checkup or screening with your doctor. Any person who knowingly and with intent to defraud any insurance. Claims for all other. Please review your policy for specific benefits covered under. Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. Short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the attached authorization. Any person who knowingly and with intent. Short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the attached authorization. Download and complete this form to file a claim for hospitalization or surgery. To avoid delays in processing of your claim form, complete each section, attaching documentation below when it applies. Primary medical. Claims for all other benefits covered under your. Do not attach receipts, statements or other claim documentation to this form. What type of coverage are you filing a claim? Schedule and complete your checkup or screening with your doctor. Please sign, date and mail/fax the completed form to the aflac. To prevent processing delays, please have claim form completed in full and return the signed American family life assurance company of columbus (aflac) attention: Short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the attached authorization. Download and complete this form to file a claim. What type of coverage are you filing a claim? Submit only one treatment date per claim form. Claims for all other benefits covered under your. Failure to complete all sections may result in a delay in processing this claim. Fill in the policy number, policyholder information, patient information, treatment and physician. Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. American family life assurance company of columbus (aflac) attention: American family life assurance company of columbus (aflac) attention: Fill in the policy number, policyholder information, patient information, treatment and physician. Find the right forms to get your claim started. American family life assurance company of columbus (aflac) attention: Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. To file your claim via fax or mail, simply download the appropriate forms below, and send to us with all necessary supporting. We're here to help you. Claims for all other benefits covered under. Any person who knowingly and with intent to defraud any insurance company, files a statement of claim containing any materially false, incomplete or misleading information, is guilty of a crime. Fill out the required information and submit the form with supporting documentation to aflac for. Submit only one treatment date per claim form. Aflac group makes it easy to file a claim. Accident claim form authorization several states require that the following statement appear on claim forms. Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. American family life assurance company of columbus (aflac) attention: To file your claim via fax or mail, simply download the appropriate forms below, and send to us with all necessary supporting. To avoid delays in processing of your claim form, complete each section, attaching documentation below when it applies. Schedule and complete your checkup or screening with your doctor. Fill in the policy number, policyholder information, patient information, treatment and physician. Attach supporting documentation, such as bills, reports, and authorization forms, and email or fax it to aflac. Please sign, date and mail/fax the completed form to the aflac. What type of coverage are you filing a claim? Claims department • worldwide headquarters • 1932 wynnton road • columbus, ga 31999 for information or help. Short term disability claim form *please attach paperwork for any additional income you are receiving during this period of disability.* **please sign and return the attached authorization.
Fillable Online Aflac Accident Wellness Claim Form Fill Online

Aflac A91195 20062021 Fill and Sign Printable Template Online US

Free Printable Aflac Wellness Claim Forms
Free Printable Aflac Wellness Claim Forms
Aflac Claim Form Medical Diagnosis Hospital
Aflac Printable Claim Forms

FREE 8 Sample Aflac Claim Forms In PDF
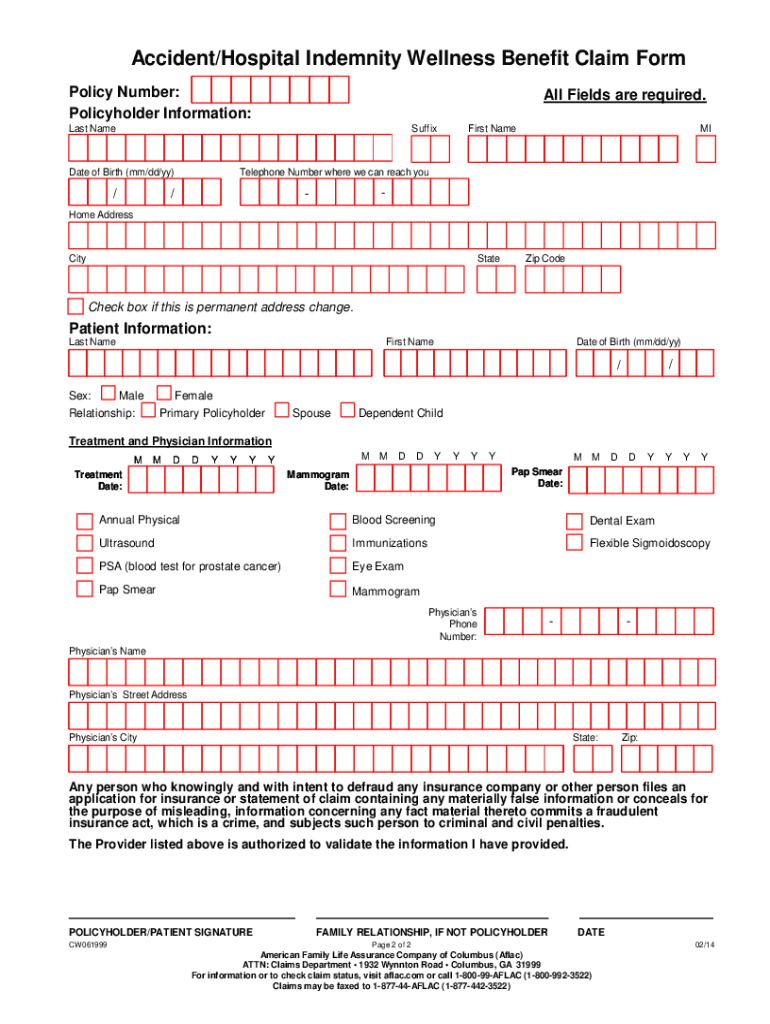
Printable Aflac Claim Forms For Mammogram
Printable Aflac Claim Forms

Aflac Claim Form Fillable Pdf Printable Forms Free Online
Download And Complete This Form To File A Claim For Hospitalization Or Surgery.
Claims Department • Worldwide Headquarters • 1932 Wynnton Road • Columbus, Ga 31999 For Information Or Help.
Follow These Five Easy Steps To File A Claim And Get Paid Fast:
Download And Print The Aflac Accidental Injury Claim Form To File A Claim For Your Policy.
Related Post: